


Cosmetic dentistry does not just create beautiful smiles with natural and youthful-looking front teeth and smiles.
It applies the most recently developed dental materials and methods to help minimize damage to tooth structure and to recreate the properties of native teeth, coining a new term: minimally invasive dentistry. The physical properties of new dental restorative materials approximate those of natural teeth. Restored teeth, including premolars and molars, look like natural teeth. Many of Dr. Rabanus older patients contact him after many years to tell him with excitement that some dentists at first look did not believe that they had anything done to their teeth. This is exactly what cosmetic dentists are striving for, naturally beautified teeth with minimum expenditure of healthy tooth structure.
It should be underlined at this point that teeth are only as "beautiful" as they are comfortable, permanent, and integrated within the framework of biological and mechanical function of the entire stomatognathic system. A tooth-colored crown for a molar does not serve any purpose, if it is not built on sound biomechanical principles as explained elsewhere in this website.
The advancement of "bonding technology" and the understanding of the way they interact with teeth and the intaglio surfaces of porcelain restorations does not just contribute to camouflaging the interfaces between teeth and dental restorations, it also produces survival rates of porcelain and composite restorations for decades. Restored teeth look and feel real, even in the back of your mouth. They can assume the same function as your natural teeth.
In addition, the development of stronger and tougher dental materials, such as eMax and zirconia products, has even facilitated the reliable and permanent rehabilitation of patients who grind their teeth or had a deteriorating masticatory system due to a variety of other reasons.
Porcelain Crowns


Composite Fillings
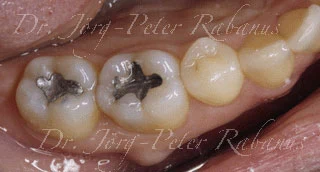
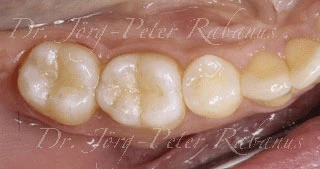
Composite Fillings


Composite Fillings & Partial Porcelain Crown

References:
Little DA et al. Occlusal parameters for ceramic restorations: biological and functional considerations. Pract Periodontics Aesthetic Dentistry 2004; 16(4); 307-311.
Lutz FU et al. dvanced adhesive restorations: the post-amalgam age. Pract Periodontics Aesthetic Dentistry 1996; 8(4); 385-394.
Radz GM. Conservative treatment planning in the posterior quadrant: the use of traditional and modern restorative materials. Pract Periodontics Aesthetic Dentistry 2004; 16(1); 17-22.
Terry DA. Clinical considerations for aesthetic laboratory-fabricated inlay/onlay restorations: a review. Pract Periodontics Aesthetic Dentistry 2001; 13(1); 51-58.
Trushkowsky R. Minimizing problems with Class II posterior composite placement. J Cosmetic Dentistry 2000; 16(2); 44-47.
Van Sternberghe D. From a fixation with teeth to a broader perspective: oral rehabilitation J Oral Rehabilitation 2004; 31; 829-830.
Trinkner TF. Achieving esthetic goals while maintaining proper bite relationships throughout treatment. Cont Esthet Rest Pract 2003; Sept; 38-50.
Yarovesky U et al. Taking Posterior Restorations to the Next Level: A New Way to Communicate Occlusal Color and Characterization. American Academy of Cosmetic Dentistry Journal 1996 Fall; 12-16.
Dawson PE. Integrating cosmetic dentistry into a complete dentistry format. J Cosmetic Dentistry 2007; 23(3); 130-134.
Dawson PE. Craniomandibular function and dysfunction. J Prosthetic Dentistry 1995; 74(6); 619-627.
Seedorf H et al. Impact of posterior occlusal support on the condylar position. J Oral Rehabilitation 2004; 31(8); 759-763.
Darveniza M. Full occlusal protection--theory and practice of occlusal therapy. Austr Dent J 2001; 46(2); 70-79.
Oh SH et al. Relationship between occlusal tooth contact patterns and tightness of proximal tooth contact. J Oral Rehabilitation 2006; 33(10); 749-753.
Okano N et al. The influence of altered occlusal guidance on condylar displacement during submaximal clenching. J Oral Rehabilitation 2005; 32(10); 714-719.
Otake T et al. The role of posterior guidances under the altered anterior guidance. J Oral Rehabilitation 2002; 29(12); 1196-1205.
Turp JC et al.Dental occlusion: a critical reflection on past, present and future concepts. J Oral Rehabilitation 2008; 35(6); 446-453.
Hanashima M et al. A study regarding occlusal plane and posterior disocclusion. Int J Stomatol Occl Med 2008; 1; 27-33
Sonnesen L et al. Molar bite force in relation to occlusion, craniofacial dimensions, and head posture in pre-orthodontic children. Eur J Orthod 2005; 27(1); 58-63.